fjrigjwwe9r0Board:Content
Sympathetic Tone
The sympathetic nervous system (flight or fight) plays an important role in C.A.D. Greater than usual sympathetic tone will increase heart rate and elevate blood pressure. Increased sympathetic activity has often been demonstrated in patients with C.A.D. Increased levels of adrenal medulla hormones, i.e., norepinephrine and epinephrine damage the arterial lining, increase platelet aggregation and increase oxidized cholesterol, all which lead to a faster generation of arthrogenesis. Remember, calcium stimulates sympathetic discharge, whereas, magnesium has antagonistic properties. Therefore, appropriate levels of magnesium and melatonin help to control an imbalanced sympathetic nervous system.
Researchers have demonstrated that patients with C.A.D. have nighttime melatonin levels that are 1/5 lower than healthy controls. Explanatory physiology is likely to be related to increased nighttime sympathetic discharge and the subsequent increase in epinephrine/norepinephrine. Also, melatonin levels could possibly explain why the majority of heart attacks occur in the early morning hours. Melatonin has also been found to inhibit platelet aggregation. Saliva melatonin sampling can be obtained from several laboratories throughout the country.

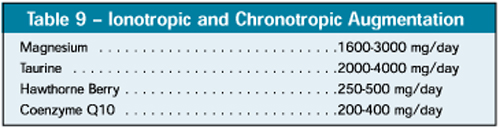
Table 9 depicts several substances with either ionotropic (increase heart contractibility) or chronotropic (rhythm heart stabilizing) effects on the heart. Regular use of these substances can often augment typical conventional medications of similar nature, i.e., digitalis and antiarrythmics. Several studies have shown magnesium to be an excellent preventative of dysrythmias and can be especially useful in intravenous doses of 2-3 gm in the early stages of heart attack and for several days thereafter. Its use can prevent the serious rhythm disturbances that often accompany myocardial infarction. Long-term use is also suggested since most patients are magnesium deficient. Other studies have determined that the use of coenzyme Q10 in dosages of 300 mg/day one week prior to cardiac surgery improves three-fold the serum levels and tissue levels in the heart of this nutraceutical. This improvement seems to reduce the heart failure associated with low coenzyme Q10. Another study on the usefulness on coenzyme Q10 in clinical cardiology demonstrated large doses over time will reduce overall cardiac medication requirements significantly. (See graphic) Taurine, an amino acid has likewise been shown to have positive cardiac effects and diuretic properties. Hawthorne berry has been used for years by western herbologists as a good ionotropic natural agent.
References
Arsenio, L., et al. Effectiveness of Long-Term Treatment with Pantethine in Patients with Dyslipidemias. Clin Ther, 1986; 8: 537-545.
Baggio, E., et al. Italian Multicenter Study on the Safety and Efficacy of Coenzyme-Q-10 as Adjunctive Therapy in Heart Failure. Co-Q-10 Drug Surveillance Investigators. Mol Aspects Med, 1994; 15 Suppl: s287-294.
Broughton, D.L., Taylor, R.L. Review: Deterioration of Glucose Tolerance with Age: The Role of Insulin Resistance: Age and Aging, 1991; 20: 221-225.
Brugger, P., et al. Impaired Nocturnal Secretion of Melatonin in Coronary Artery Disease. Lancet, 1995; 345: 1408.
Cantin, B., et al. Lipoprotein (a) An Independent Risk Factor for Ischemic Heart Disease in Men? The Quebec Cardiovascular Study. J Am Cardiol, 1998; 31:519-525.
Cardinali, D.P., Del Zar, M.M., Vacas, M.I. The Effects of Melatonin in Human Platelets. Acta Physiol Pharmacol Ther Latinoam, 1993; 43: 1-13.
Chappell, L.T., Stahl, J.P. The Correlation Between EDTA Chelation Therapy and Improvement in Cardiovascular Function: A Meta-Analysis. J Adv Med, 1993; 6: 139-160.
Dabbs, J.M. Savory Testosterone Measurements: Collecting, Storing and Mailing Saliva Samples. Physiology and Behavior, 1991; 49: 815-817.
El-Enein Ama, et al. The Role of Nicotinic Acid and Inositol Hexanicotinate as Anti-Cholesterolemic and Anti-lipemic Agents. Nutr Rep Intl, 1983; 28: 899-911.
Folsom, A. Homocysteine: Not a Risk Factor. Circulation 98, 1998; 196-199, 204-210.
Fox, M. More Evidence that Infections Cause Heart Disease. Science News, Sept 18, 2000.
Fukagawa, N.K., Anderson, J.W., et al. High-Carbohydrate, High Fiver Diets Increase Peripheral Insulin Sensitivity in Healthy Young and Old Adults. Am J Clin Nutr, 1990; 52: 524-528.
Ghen, M.J., et al. The Advanced Guide to Longevity Medicine. 2001, Landrum, South Carolina, pp. 193-201, 239-246.
Graham, I.M., et al. Plasma Homocysteine as a Risk Factor for Vascular Disease: The European Concerted Action Project. JAMA, 1997; 277; 1775-1781.
Hancke, C., Flytlie, K. Benefits of EDTA Chelation Therapy in Arteriosclerosis: A Retrospective Study of 47- Patients. Journal of Advancement in Medicine, 1993; 6(3); 161-172.
Langsjoen, H., et al. Usefulness of Coenzyme-Q-10 in Clinical Cardiology: A Long Term Study. Mol Aspects Med, 1994; 15 Suppl: s165-175.
Lipson, S.F., Ellison, P.T. Development of Protocols for the Application of Salivary Steroid Analysis to Field Conditions. American Journal of Human Biology, 1989; 1:249-255.
Lukaczer, Dan. Nutritional Support for Insulin Resistance. Applied Nutritional Science Reports, July 2001; pp. 1-6.
Maurer HR. Bromelain: biochemistry, pharmacology and medical use. Cell Mol Life Sci 2001;58:1234-45.
Merghioli, Robert, et al. Dietary Supplementation with N-3 Polyunsaturated Fatty Acids and Vitamin E After Myocardial Infarction: Results of the GISSI-PREVENZIONE Trial. The Lancet, Volume 234, Aug 7, 1999; pp 447-495.
Mori, T.A., et al. Interactions Between Dietary Fat, Fish, and Fish Oils and their Effects on Platelet Function Men at Risk with Cardiovascular Disease. Arterioscler Throm Vasc Biol, 1997; 17:279-286.
Phillips, R., Lemon, F., Kuzma, J. Coronary Heart Disease, Mortality Among Seventh Day Adventists with Differing Dietary Habits. Am J Clin Nutr, 1978 Oct 31;(10 Suppl): 5191-5198.
Rosenfeldt, Franklin, et al. Experience with Coenzyme-Q-10 in Cardiac Surgery Patients. 2nd Conference of the International Co-Q-10 Association. Frankfurt, Germany, December 1-3, 2000.
Watson, P.S., Scalia, G.M., et al. Lack of effect of Coenzyme-Q-10 on Left Ventricular Function in Patients with Congestive Heart Failure. J Am Coll Cardiol, 1999, May; 33(6):1549-1552.
Weiss, Decker. Part One: Cardiovascular Disease Risk Factors and Fundamental Nutrition. Applied Nutritional Science Reports, Feb 2000, pp. 1-6.
Welsh, A.L, Edede, M. Inositol Hexanicotinate for Improved Nicotinic Acid Therapy. Int Record Med, 1961; 174:9-15.
Weiss, Decker. Part Two: Cardiovascular Disease Nutrtional Management of Clinical Markers. Applied Nutritional Science Reports, Feb 2000, pp. 1-6. |















 > Seminar & Notice > Seminar
> Seminar & Notice > Seminar










