Traditional Medical Treatments
- In order to survive, people with type 1 diabetes must have insulin delivered by a pump or injections.
- Many people with type 2 diabetes can control their blood glucose by following a careful diet and exercise program, losing excess weight, and if needed taking oral medication. It is important to strive to educate patients about the beneficial nutritional and physiological aspects of treatment. Many times these treatments are overlooked by the medical profession, or minimal time is spent on these recommendations in lieu of writing a prescription medication as a first line treatment.
- Traditional physicians may treat people with diabetes with several medications to control their cholesterol and blood pressure in an effort to prevent premature cardiac and renal complications.
- Among adults with diagnosed diabetes, about 11 percent take both insulin and oral medications, 22 percent take insulin only, 49 percent take oral medications only, and 17 percent do not take either insulin or oral medications.
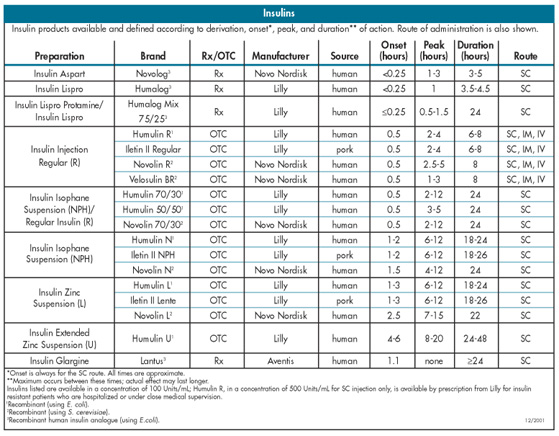
The various insulins and oral medications for type 2 diabetes are listed in the table titled "Insulins."
Classes of diabetic medications
Physicians have five different "classes" of oral prescription drugs which can be used to treat type 2 diabetes and injectable insulin. Several of these oral medications have just been recently released for widespread use.
Sulfonylureas
The long standing class of drugs, the sulfonylureas, have been the mainstay of the oral medications for many years. Sulfonylureas have been used for the treatment of type 2 diabetes since the 1950's. Acetohexamide (Dymelor), Tolbutamide (Orinase) and Tolazamide (Tolinase) were all first- generation sulfonylureas. Diabinase or chlorpropamide, was one the newer sulfonylureas, which like its first-generation cousins, has some major drawbacks when treating diabetes. This class has a tendency to put weight on patients and also cause low blood sugar levels. Low blood sugar, called hypo-glycemia, occurs when the blood glucose falls below a certain level and causes several symptoms. Signs of hypoglycemia include mental confusion, dizziness, loss of consciousness and others. This is precisely the opposite effect that we wish to see. We want people with diabetes to lose those unnecessary pounds, not accumulate more! Insulin has at times been necessary to treat patients with type 2 diabetes. Naturally, patients would not prefer this type of treatment due to the invasive nature of daily injections, so the oral agents are more popular when they work to lower blood glucose levels. The sulfonylureas also increase insulin levels by directly stimulating release. There are currently seven of them to choose from, of which the latest three to come to market are called "second generation" sulfony-lureas. These latest "offspring" are glyburide (Micronase, Glynase and Diabeta), glipizide (Glucotrol, Glucotrol XL) and the youngest brother glimepiride (Amaryl). Sulfonylureas stimulate more insulin release, however many times the insulin levels are already elevated, thus compounding the problems that are associated with increased insulin levels.
The newer prescriptions for type 2 diabetes are:
Acarbose (Precrose) an [alpha-glucosidase inhibitor]
The alpha-glucosidase inhibitors such as Acarbose are best used to treat the elevated glucose levels which occur after eating in diabetic patients. This medication is better for carbohydrate intolerance and is better than sulfonylureas which can promote a rapid drop in glucose levels causing low blood sugar and magnify other medical problems. This drug was released for use in 1996 but was used prior to this in Canada and in Europe. Glyset is the newest of the AGI's.
Ascarbose interferes with an enzyme called alpha-glucosidase in the small intestine. This enzyme is responsible for breaking down various ingested sugars in the small intestine. If they are not able to be broken down, they cannot be absorbed and the blood glucose level is less likely to rise abnormally after eating. This blocks glucose uptake from the small intestine but carries with it some pretty unfriendly side effects. Excessive gas and flatulence, diarrhea and abdominal pain make it a questionable drug to use without the fear of a social "accident." Elevated liver function test can also occur with Ascarbose. Particular care must be taken as a hypoglycemic event must be treated with oral tablets or gel due to the absorption blocking activity in the small intestine. Patients with inflammatory bowel problems, such as irritable bowel disease, ulcers and colitis should also refrain from this alternative treatment. Patients with kidney problems should also look elsewhere for type 2 medication.
Metformin (Glucophage) a [biguanide]
The biguanids, like metformin, are improved diabetic drugs as they do not cause weight gain like the sulfonylureas, nor do they increase cardiovascular risk profiles. Metformin causes the liver and the muscle to utilize glucose better. In the muscles, metformin causes glucose to get into the cells more easily to be metabolized. It also causes the liver to slow down production of glucose. Glucophage was introduced in the spring of 1995 and has been shown to lower triglyceride levels, as well as total and LDL cholesterol levels. It also causes a rise in the good cholesterol levels (HDL cholesterol) with a slight loss of weight.
The benefits of this medication however have their costs. People taking the medication report bloating, nausea, cramps, abdominal fullness and diarrhea as the unpleasant side effects. They do, however, usually go away after several days. Patients with kidney problems or congestive heart failure are not to take this medication, nor are any patients with liver problems. Alcohol and binge drinking are not to be mixed with metformin. It should not be taken within 48 hours after any tests which use iodine as the contrast material such as an IVP or CT scan.
Troglitazone (Rezulin) a [thiazolidinedione]
One of the newest medications for diabetes is a thiazo-lidinedione called Troglitazone or Rezulin, which was taken off the market just after its debut. This medication was the first medication which worked directly on insulin resistance. Rezulin increases the effect of insulin, but not the actual release of the hormone. Th















 > Seminar & Notice > Seminar
> Seminar & Notice > Seminar










